Loading
Get Dental Claim Form 2013-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Dental Claim Form online
Filling out the Dental Claim Form online can streamline the process of submitting your dental expenses for reimbursement. This guide will provide you with clear, step-by-step instructions to ensure your form is completed accurately and efficiently.
Follow the steps to complete your Dental Claim Form online
- Click ‘Get Form’ button to access the Dental Claim Form and open it in your preferred document editor.
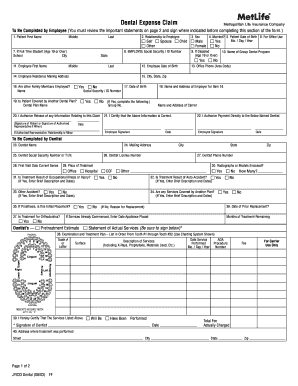
- Begin by filling out the patient's information. Enter the patient's first name, middle initial, and last name in the designated fields.
- Indicate the relationship of the patient to the employee. Choose from the options provided, such as self, spouse, or child.
- Select the patient's sex by checking either the male or female box.
- Indicate whether the patient is married by selecting yes or no.
- Input the patient's date of birth in the format Mo./Day/Year.
- If applicable, provide information about the patient’s school and city if they are a full-time student aged 19 or over.
- Fill in the employee's social security or ID number in item 8. This information is crucial for processing the claim.
- If the patient is disabled, indicate this by checking yes or no.
- Enter the name of the group dental program, if applicable.
- Next, input the employee's information. Include their first name, middle initial, last name, and date of birth.
- Provide the employee's mailing address, including city, state, and zip code.
- Indicate whether other family members are employed by checking yes or no.
- Fill in the name and address of the employer for item 16.
- If the patient is covered by another dental plan, select yes and complete the related fields. Otherwise, check the no option.
- Authorize the release of information related to the claim by signing where indicated.
- Certify the accuracy of the information by signing the designated section.
- If applicable, specify if you want payment to be made directly to the dentist by completing item 22.
- Review all entered information for completeness and accuracy.
- Once complete, save the changes to the form, and consider downloading or printing a copy for your records.
Take action now by filling out your Dental Claim Form online to ensure timely reimbursement for your dental expenses.
Filling out claim form part A requires you to provide personal information such as your name, address, and insurance policy number. It is important to enter this information clearly and accurately to avoid delays. Always double-check for completeness, as a well-filled claim form will streamline the approval process.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.