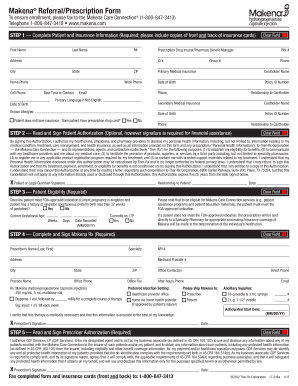
Get Makena Prescription Form
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign PRETERM online
How to fill out and sign Npi online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
The prep of legal paperwork can be costly and time-consuming. However, with our pre-built online templates, everything gets simpler. Now, creating a Prescription Form requires a maximum of 5 minutes. Our state-specific online samples and complete instructions eradicate human-prone faults.
Comply with our simple actions to have your Prescription Form well prepared quickly:
- Find the web sample from the library.
- Enter all necessary information in the required fillable areas. The intuitive drag&drop interface allows you to include or relocate fields.
- Ensure everything is completed appropriately, with no typos or lacking blocks.
- Place your e-signature to the page.
- Click on Done to confirm the alterations.
- Download the record or print out your PDF version.
- Distribute immediately towards the receiver.
Use the quick search and advanced cloud editor to produce a correct Prescription Form. Get rid of the routine and produce paperwork online!
How to edit 18-g: customize forms online
Have your stressless and paper-free way of working with 18-g. Use our trusted online solution and save a lot of time.
Drafting every form, including 18-g, from scratch takes too much time, so having a tried-and-true platform of pre-uploaded document templates can do wonders for your productivity.
But working with them can be problem, especially when it comes to the files in PDF format. Fortunately, our extensive library has a built-in editor that lets you easily fill out and edit 18-g without leaving our website so that you don't need to waste time completing your documents. Here's what you can do with your document utilizing our solution:
- Step 1. Locate the required document on our website.
- Step 2. Hit Get Form to open it in the editor.
- Step 3. Use our professional editing features that let you insert, remove, annotate and highlight or blackout text.
- Step 4. Generate and add a legally-binding signature to your document by utilizing the sign option from the top toolbar.
- Step 5. If the form layout doesn’t look the way you need it, utilize the features on the right to erase, add more, and arrange pages.
- step 6. Add fillable fields so other persons can be invited to fill out the form (if applicable).
- Step 7. Pass around or send the form, print it out, or choose the format in which you’d like to download the file.
Whether you need to execute editable 18-g or any other form available in our catalog, you’re on the right track with our online document editor. It's easy and secure and doesn’t require you to have special tech background. Our web-based solution is set up to deal with virtually everything you can imagine concerning file editing and execution.
No longer use conventional way of handling your documents. Go with a a professional solution to help you streamline your tasks and make them less reliant on paper.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Caproate FAQ
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to Prescription Form
- fda
- prescriber
- StateZIP
- yy
- Hydroxyprogesterone
- 17P
- caproate
- 17-246a
- PRETERM
- Plano
- redisclosed
- npi
- 18-g
- ome
- tx
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

