Get Tb Screening Questionnaire
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
Tips on how to fill out, edit and sign Printable tb test screening form online
How to fill out and sign Tb screening questionnaire form online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
Feel all the advantages of completing and submitting legal forms online. Using our platform submitting TB Screening Questionnaire will take a few minutes. We make that possible through giving you access to our full-fledged editor capable of altering/fixing a document?s initial text, adding special fields, and e-signing.
Fill out TB Screening Questionnaire in just several moments by following the recommendations listed below:
- Find the document template you need from our collection of legal form samples.
- Click on the Get form key to open the document and start editing.
- Fill in the required boxes (they will be marked in yellow).
- The Signature Wizard will allow you to add your e-signature as soon as you have finished imputing information.
- Add the relevant date.
- Check the whole form to be certain you have completed all the information and no changes are required.
- Hit Done and download the resulting template to your gadget.
Send the new TB Screening Questionnaire in an electronic form when you are done with completing it. Your information is well-protected, because we keep to the most up-to-date security criteria. Join numerous satisfied users who are already submitting legal templates right from their homes.
How to edit Tb screening tool: customize forms online
Use our comprehensive editor to transform a simple online template into a completed document. Read on to learn how to modify Tb screening tool online easily.
Once you discover an ideal Tb screening tool, all you have to do is adjust the template to your needs or legal requirements. Apart from completing the fillable form with accurate data, you may want to delete some provisions in the document that are irrelevant to your circumstance. Alternatively, you might like to add some missing conditions in the original template. Our advanced document editing tools are the best way to fix and adjust the document.
The editor lets you change the content of any form, even if the file is in PDF format. It is possible to add and remove text, insert fillable fields, and make additional changes while keeping the original formatting of the document. Also you can rearrange the structure of the form by changing page order.
You don’t have to print the Tb screening tool to sign it. The editor comes along with electronic signature capabilities. Most of the forms already have signature fields. So, you just need to add your signature and request one from the other signing party with a few clicks.
Follow this step-by-step guide to build your Tb screening tool:
- Open the preferred template.
- Use the toolbar to adjust the form to your preferences.
- Fill out the form providing accurate information.
- Click on the signature field and add your eSignature.
- Send the document for signature to other signers if needed.
After all parties complete the document, you will receive a signed copy which you can download, print, and share with other people.
Our services let you save tons of your time and minimize the chance of an error in your documents. Streamline your document workflows with efficient editing tools and a powerful eSignature solution.
Related links form
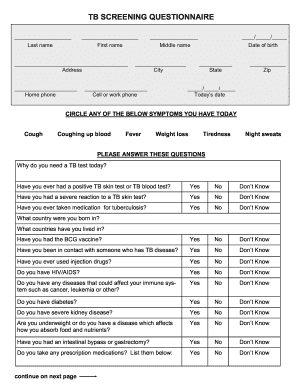
A TB screening test is performed by administering either a skin or blood test to assess for TB infection. After completing the TB Screening Questionnaire, a health professional will conduct the test, followed by a required waiting period for reading the results. The results provide critical information regarding your TB health status, guiding any further actions needed. Rely on uslegalforms for assistance in managing any required paperwork.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.