Get Medical History Form
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign Health history update form dental online
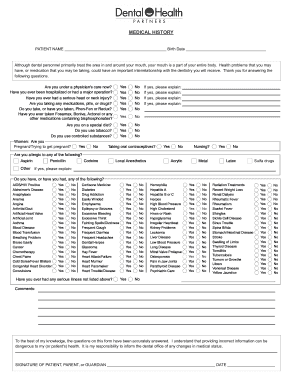
How to fill out and sign Medical history form dental online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
The days of frightening complex tax and legal documents are over. With US Legal Forms creating official documents is anxiety-free. A powerhouse editor is already close at hand offering you a wide range of useful tools for submitting a Dental Health Medical History Form. These guidelines, in addition to the editor will help you with the complete process.
- Hit the Get Form option to start enhancing.
- Activate the Wizard mode in the top toolbar to obtain more recommendations.
- Fill each fillable field.
- Be sure the details you add to the Dental Health Medical History Form is updated and correct.
- Indicate the date to the sample with the Date option.
- Click the Sign tool and make an e-signature. You can find 3 available alternatives; typing, drawing, or capturing one.
- Be sure that every area has been filled in correctly.
- Select Done in the top right corne to save the sample. There are various options for receiving the doc. As an instant download, an attachment in an email or through the mail as a hard copy.
We make completing any Dental Health Medical History Form less difficult. Use it now!
How to edit Medical history forms: customize forms online
Have your stressless and paper-free way of modifying Medical history forms. Use our reliable online option and save a lot of time.
Drafting every document, including Medical history forms, from scratch takes too much time, so having a tried-and-true platform of pre-uploaded document templates can do wonders for your efficiency.
But modifying them can be struggle, especially when it comes to the files in PDF format. Luckily, our extensive catalog has a built-in editor that allows you to easily complete and customize Medical history forms without the need of leaving our website so that you don't need to waste hours executing your forms. Here's what you can do with your form using our tools:
- Step 1. Find the needed document on our website.
- Step 2. Click Get Form to open it in the editor.
- Step 3. Take advantage of professional modifying tools that let you add, remove, annotate and highlight or blackout text.
- Step 4. Generate and add a legally-binding signature to your form by utilizing the sign option from the top toolbar.
- Step 5. If the document layout doesn’t look the way you want it, utilize the tools on the right to erase, put, and re-order pages.
- step 6. Add fillable fields so other persons can be invited to complete the document (if applicable).
- Step 7. Share or send the document, print it out, or choose the format in which you’d like to download the document.
Whether you need to execute editable Medical history forms or any other document available in our catalog, you’re on the right track with our online document editor. It's easy and safe and doesn’t require you to have particular skills. Our web-based tool is set up to deal with virtually everything you can think of when it comes to document editing and execution.
No longer use conventional way of working with your forms. Choose a more efficient solution to help you simplify your tasks and make them less dependent on paper.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Video instructions and help with filling out and completing medical history form pdf
Find out about the best way to complete Form on the web. Use our video guide to understand why going digital is the best way to manage documents in 2020 and beyond.
Medical history form print FAQ
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to medical history form sample
- aesthetics medical history form
- the written medical dental health history form
- dental medical history update form
- history medical form
- medical history form dental sample
- dental medical history update form template
- medical history form dental printable
- medical history template
- medical history form printable
- medical history form dental pdf
- medical history form blank
- medical history form online
- medical history form for microblading
- medical history form dental template
- medical history form for dental office
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

