Get Novo Nordisk Refill Form
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign Novolog medication template online
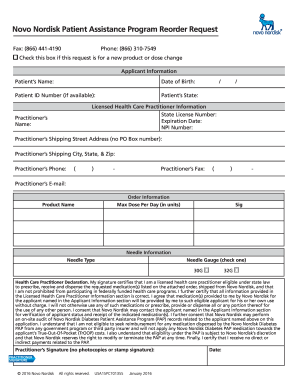
How to fill out and sign Novo nordisk patient assistance form online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
Feel all the benefits of submitting and completing documents online. Using our service filling in Novo Nordisk Patient Assistance Refill Form 2020 usually takes a few minutes. We make that possible by giving you access to our feature-rich editor capable of altering/correcting a document?s initial text, inserting special boxes, and putting your signature on.
Execute Novo Nordisk Patient Assistance Refill Form 2020 within a couple of minutes by using the instructions listed below:
- Pick the template you want from the library of legal form samples.
- Click the Get form button to open the document and move to editing.
- Complete the required fields (they will be yellowish).
- The Signature Wizard will enable you to add your e-signature after you have finished imputing info.
- Add the relevant date.
- Look through the whole form to make sure you have filled out all the information and no changes are required.
- Hit Done and download the resulting template to your device.
Send your new Novo Nordisk Patient Assistance Refill Form 2020 in a digital form when you finish completing it. Your information is well-protected, since we keep to the newest security requirements. Join millions of satisfied users who are already submitting legal forms right from their apartments.
How to edit Ozempic pt assistance: customize forms online
Your easily editable and customizable Ozempic pt assistance template is within reach. Make the most of our library with a built-in online editor.
Do you postpone completing Ozempic pt assistance because you simply don't know where to begin and how to move forward? We understand how you feel and have an excellent tool for you that has nothing nothing to do with overcoming your procrastination!
Our online catalog of ready-to-use templates lets you search through and choose from thousands of fillable forms adapted for various use cases and scenarios. But getting the form is just scratching the surface. We offer you all the needed features to fill out, sign, and change the form of your choice without leaving our website.
All you need to do is to open the form in the editor. Check the verbiage of Ozempic pt assistance and confirm whether it's what you’re searching for. Begin modifying the form by taking advantage of the annotation features to give your form a more organized and neater look.
- Add checkmarks, circles, arrows and lines.
- Highlight, blackout, and fix the existing text.
- If the form is intended for other users too, you can add fillable fields and share them for other parties to fill out.
- Once you’re through modifying the template, you can download the document in any available format or choose any sharing or delivery options.
Summing up, along with Ozempic pt assistance, you'll get:
- A robust set of editing} and annotation features.
- A built-in legally-binding eSignature functionality.
- The option to create forms from scratch or based on the pre-drafted template.
- Compatibility with different platforms and devices for increased convenience.
- Many possibilities for safeguarding your files.
- A wide range of delivery options for easier sharing and sending out files.
- Compliance with eSignature frameworks regulating the use of eSignature in online operations.
With our professional tool, your completed forms are always officially binding and completely encoded. We make certain to safeguard your most hypersensitive information and facts.
Get all it takes to generate a professional-seeking Ozempic pt assistance. Make the best choice and attempt our program now!
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Novo refill form FAQ
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to novolog patient assistance refill reorder request
- novonordisk patient assistance program refill
- novo nordisk refill form 2022
- ozempic patient assistance form pdf
- novo nordisk refill
- 2022 novo nordisk patient assistance refill reorder change form
- novo nordisk pt assistance form
- novo nordisk pt assistance
- novo nordisk patient assistance ozempic
- lantus patient assistance refill form
- new novo nordisk refill form
- novo dose increase form
- novo forms
- novo nordisk pap
- novo nordisk pap refill form 2022
- novo nordisk pap reorder pdf
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

