Get Wi F-44192 2017
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign 3rd online
How to fill out and sign 5th online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
Feel all the advantages of submitting and completing legal forms on the internet. Using our platform submitting WI F-44192 only takes a couple of minutes. We make that achievable through giving you access to our feature-rich editor capable of transforming/correcting a document?s initial text, inserting special boxes, and e-signing.
Complete WI F-44192 in a few minutes following the recommendations below:
- Choose the document template you want from our collection of legal form samples.
- Click on the Get form key to open the document and begin editing.
- Complete all of the necessary fields (they are marked in yellow).
- The Signature Wizard will help you put your electronic signature right after you?ve finished imputing information.
- Insert the date.
- Look through the entire template to be certain you have completed all the information and no corrections are needed.
- Click Done and save the ecompleted template to your computer.
Send the new WI F-44192 in a digital form when you finish completing it. Your data is securely protected, since we adhere to the most up-to-date security requirements. Become one of numerous happy users who are already filling in legal forms right from their homes.
How to edit HIB1: customize forms online
Take advantage of the usability of the multi-featured online editor while filling out your HIB1. Make use of the variety of tools to rapidly complete the blanks and provide the requested information right away.
Preparing documents is time-taking and pricey unless you have ready-made fillable forms and complete them electronically. The easiest way to cope with the HIB1 is to use our professional and multi-featured online editing solutions. We provide you with all the necessary tools for fast form fill-out and enable you to make any edits to your templates, adapting them to any needs. Besides that, you can comment on the changes and leave notes for other people involved.
Here’s what you can do with your HIB1 in our editor:
- Fill out the blank fields using Text, Cross, Check, Initials, Date, and Sign options.
- Highlight essential details with a desired color or underline them.
- Hide confidential data using the Blackout tool or simply remove them.
- Add pictures to visualize your HIB1.
- Substitute the original text using the one corresponding with your needs.
- Add comments or sticky notes to inform others about the updates.
- Place extra fillable fields and assign them to exact recipients.
- Protect the template with watermarks, add dates, and bates numbers.
- Share the paperwork in various ways and save it on your device or the cloud in different formats after you finish modifying.
Working with HIB1 in our powerful online editor is the fastest and most effective way to manage, submit, and share your paperwork the way you need it from anywhere. The tool works from the cloud so that you can utilize it from any location on any internet-connected device. All templates you generate or prepare are securely kept in the cloud, so you can always access them whenever needed and be assured of not losing them. Stop wasting time on manual document completion and get rid of papers; make it all online with minimum effort.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Video instructions and help with filling out and completing MMR
Make use of our fast video information for finishing Form in your browser. Turning to paperless is the only way to save your time for more crucial activities in the digital age.
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
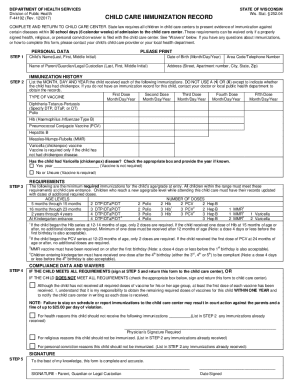
Keywords relevant to WI F-44192
- Varicella
- MMR3
- childs
- 4th
- MMR
- 1st
- PCV2
- Rubella
- 3rd
- influenzae
- Haemophilus
- 5th
- HIB1
- Pneumococcal
- pertussis
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

