Get Ca Medical Board Form 071-61 2020-2025
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign Medical board format online
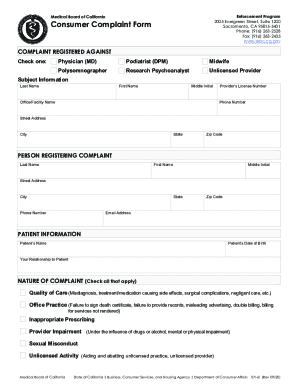
How to fill out and sign California medical board complaint form online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
The days of terrifying complicated legal and tax documents have ended. With US Legal Forms the entire process of creating legal documents is anxiety-free. The best editor is right close at hand providing you with multiple beneficial tools for completing a CA Medical Board Form 071-61. These guidelines, in addition to the editor will guide you with the complete process.
- Hit the Get Form button to begin enhancing.
- Activate the Wizard mode on the top toolbar to get additional pieces of advice.
- Fill in each fillable field.
- Ensure that the information you add to the CA Medical Board Form 071-61 is up-to-date and accurate.
- Indicate the date to the template using the Date function.
- Click the Sign tool and create a signature. You can use three available alternatives; typing, drawing, or uploading one.
- Double-check each field has been filled in correctly.
- Select Done in the top right corne to save the document. There are many choices for getting the doc. An attachment in an email or through the mail as a hard copy, as an instant download.
We make completing any CA Medical Board Form 071-61 less difficult. Get started now!
How to edit Medical board complaints: customize forms online
Choose the right Medical board complaints template and modify it on the spot. Simplify your paperwork with a smart document editing solution for online forms.
Your day-to-day workflow with documents and forms can be more effective when you have everything required in one place. For instance, you can find, get, and modify Medical board complaints in one browser tab. Should you need a specific Medical board complaints, you can easily find it with the help of the smart search engine and access it right away. You do not need to download it or look for a third-party editor to modify it and add your details. All the tools for efficient work go in one packaged solution.
This modifying solution allows you to modify, fill, and sign your Medical board complaints form right on the spot. Once you see a suitable template, click on it to go to the modifying mode. Once you open the form in the editor, you have all the needed tools at your fingertips. You can easily fill in the dedicated fields and remove them if needed with the help of a simple yet multifunctional toolbar. Apply all the modifications right away, and sign the form without leaving the tab by simply clicking the signature field. After that, you can send or print your file if required.
Make more custom edits with available tools.
- Annotate your file using the Sticky note tool by putting a note at any spot within the document.
- Add required graphic elements, if required, with the Circle, Check, or Cross tools.
- Modify or add text anywhere in the document using Texts and Text box tools. Add content with the Initials or Date tool.
- Modify the template text using the Highlight and Blackout, or Erase tools.
- Add custom graphic elements using the Arrow and Line, or Draw tools.
Discover new possibilities in efficient and simple paperwork. Find the Medical board complaints you need in minutes and fill it out in in the same tab. Clear the mess in your paperwork for good with the help of online forms.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Video instructions and help with filling out and completing california medical board complaint
Go digital, complete and adjust your Form in your browser utilizing expert-made samples. This video guide will provide you with all the information and know-how you need to get started now.
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to patient complaint form health care
- medical malpractice complaint form
- medical grievance form
- medical complaint form
- medical complaint board
- board consumer complaint
- board form complaint
- medical board of california
- board medical complaint
- medical board complaints california
- ca form complaint
- mbc complaint
- how to file a complaint against a doctor in california
- ca medical complaint
- file complaint against doctor
- california board complaint
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

