Get Ca E3065 2015
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign Blank e3065 form online
How to fill out and sign State fund medical mileage expense form online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
The preparation of lawful documents can be costly and time-ingesting. However, with our pre-built online templates, things get simpler. Now, creating a CA e3065 takes no more than 5 minutes. Our state online blanks and complete recommendations eliminate human-prone faults.
Follow our simple actions to have your CA e3065 prepared rapidly:
- Choose the template in the library.
- Complete all necessary information in the required fillable fields. The easy-to-use drag&drop interface makes it easy to add or move fields.
- Check if everything is filled out properly, without typos or missing blocks.
- Apply your e-signature to the page.
- Simply click Done to confirm the changes.
- Save the data file or print out your PDF version.
- Distribute instantly to the receiver.
Make use of the fast search and powerful cloud editor to generate a correct CA e3065. Eliminate the routine and produce documents on the internet!
How to edit State fund forms: customize forms online
Choose the right State fund forms template and modify it on the spot. Simplify your paperwork with a smart document editing solution for online forms.
Your daily workflow with documents and forms can be more effective when you have everything required in one place. For example, you can find, get, and modify State fund forms in one browser tab. Should you need a specific State fund forms, it is simple to find it with the help of the smart search engine and access it immediately. You don’t have to download it or look for a third-party editor to modify it and add your data. All the resources for efficient work go in one packaged solution.
This modifying solution enables you to customize, fill, and sign your State fund forms form right on the spot. Once you find a suitable template, click on it to open the modifying mode. Once you open the form in the editor, you have all the necessary instruments at your fingertips. It is easy to fill in the dedicated fields and remove them if necessary with the help of a simple yet multifunctional toolbar. Apply all the changes immediately, and sign the form without leaving the tab by simply clicking the signature field. After that, you can send or print out your file if needed.
Make more custom edits with available instruments.
- Annotate your file using the Sticky note tool by putting a note at any spot within the document.
- Add required visual components, if required, with the Circle, Check, or Cross instruments.
- Modify or add text anywhere in the document using Texts and Text box instruments. Add content with the Initials or Date tool.
- Modify the template text using the Highlight and Blackout, or Erase instruments.
- Add custom visual components using the Arrow and Line, or Draw tools.
Discover new options in efficient and trouble-free paperwork. Find the State fund forms you need in minutes and fill it out in in the same tab. Clear the mess in your paperwork once and for all with the help of online forms.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Video instructions and help with filling out and completing state compensation insurance fund form e3065
Get your Form filled out and e-signed from the safely at home. This video shows you how to prepare and handle legal documents remotely.
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to CA e3065
- state fund workers compensation mileage forms
- scif 2019 mileage form
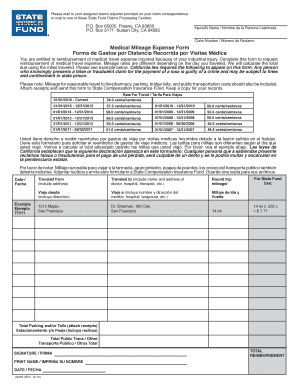
- scif medical mileage expense form
- scif mileage form
- state compensation insurance fund form e3065
- canada worksafebc occupational first aid patient create
- state fund medical mileage form
- scif form e3065
- blank e3065 form
- state fund forms e3065
- e3065
- state fund medical mileage expense form
- state fund forms
- state fund mileage form
- state fund mileage
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

