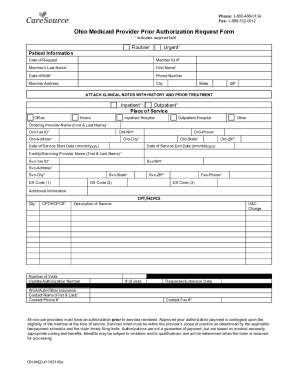
Get Oh Caresource Medicaid Provider Prior Authorization Request Form 2021-2025
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Tips on how to fill out, edit and sign Limitation online
How to fill out and sign OUTPATIENT online?
Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Follow the simple instructions below:
Are you seeking a fast and practical tool to fill in OH CareSource Medicaid Provider Prior Authorization Request Form at a reasonable cost? Our platform gives you an extensive collection of forms that are available for filling out on the internet. It only takes a couple of minutes.
Follow these simple instructions to get OH CareSource Medicaid Provider Prior Authorization Request Form completely ready for submitting:
- Get the form you will need in our library of legal templates.
- Open the form in our online editing tool.
- Read the recommendations to discover which data you will need to give.
- Select the fillable fields and add the requested details.
- Put the relevant date and place your electronic autograph once you complete all other boxes.
- Check the completed document for misprints along with other errors. If there?s a necessity to change some information, the online editor as well as its wide range of tools are available for you.
- Download the completed template to your computer by clicking Done.
- Send the e-document to the intended recipient.
Filling out OH CareSource Medicaid Provider Prior Authorization Request Form doesn?t need to be stressful anymore. From now on simply get through it from your home or at the business office straight from your mobile or personal computer.
How to edit Servicing: customize forms online
Use our advanced editor to turn a simple online template into a completed document. Continue reading to learn how to modify Servicing online easily.
Once you find a perfect Servicing, all you have to do is adjust the template to your needs or legal requirements. Apart from completing the fillable form with accurate details, you may need to delete some provisions in the document that are irrelevant to your circumstance. Alternatively, you might like to add some missing conditions in the original form. Our advanced document editing tools are the best way to fix and adjust the document.
The editor lets you modify the content of any form, even if the file is in PDF format. It is possible to add and erase text, insert fillable fields, and make extra changes while keeping the initial formatting of the document. Also you can rearrange the structure of the document by changing page order.
You don’t have to print the Servicing to sign it. The editor comes along with electronic signature capabilities. Most of the forms already have signature fields. So, you only need to add your signature and request one from the other signing party with a few clicks.
Follow this step-by-step guide to build your Servicing:
- Open the preferred form.
- Use the toolbar to adjust the template to your preferences.
- Complete the form providing accurate information.
- Click on the signature field and add your electronic signature.
- Send the document for signature to other signers if needed.
After all parties sign the document, you will get a signed copy which you can download, print, and share with other people.
Our services let you save tons of your time and reduce the chance of an error in your documents. Enhance your document workflows with effective editing tools and a powerful eSignature solution.
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
ELIGIBILITY FAQ
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to OH CareSource Medicaid Provider Prior Authorization Request Form
- qty
- 743150a
- FAC
- Authorizations
- cpt
- inpatient
- ELIGIBILITY
- applicable
- limitation
- Providers
- ord
- OUTPATIENT
- servicing
- billed
- medicaid
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

