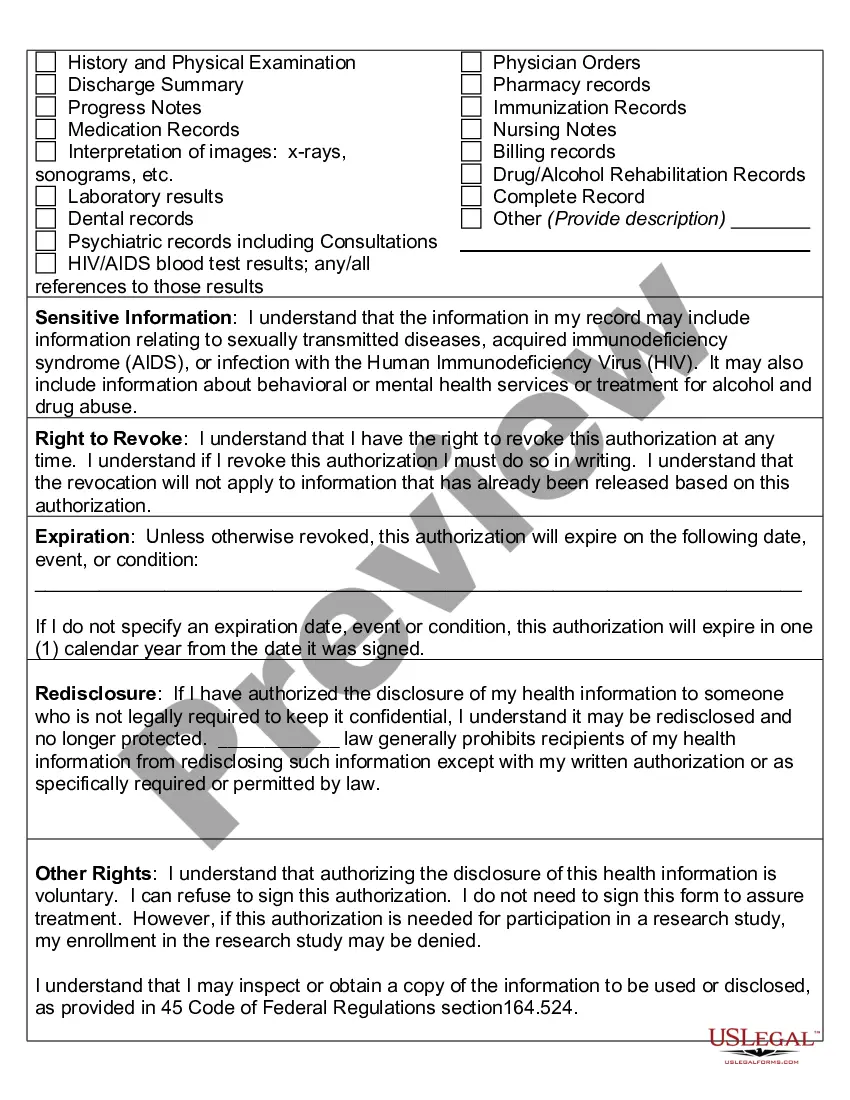
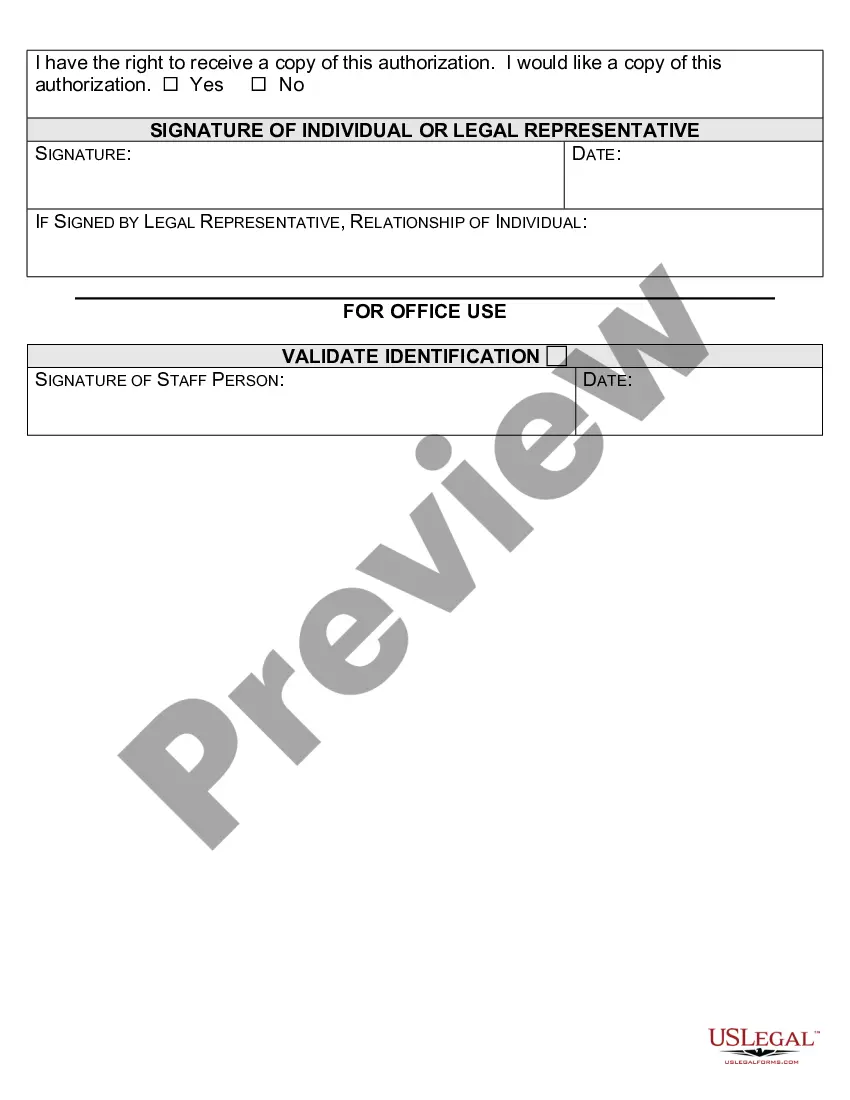
Kentucky Authorization to Use or Disclose Protected Health Information (PHI) is a legal document that grants healthcare professionals the authority to share an individual's confidential medical information with third parties. This authorization ensures compliance with the Health Insurance Portability and Accountability Act (HIPAA), which protects patients' privacy rights and regulates the use and disclosure of PHI. The Kentucky Authorization to Use or Disclose PHI includes specific details about the purpose of the disclosure, the healthcare entities involved, and the type of information being shared. It requires the patient's explicit consent, usually obtained through their signature on the authorization form. This process allows healthcare providers to share an individual's PHI in situations such as coordination of care, billing and insurance claims, research studies, or legal proceedings. There are different types of Kentucky Authorization to Use or Disclose PHI, depending on the specific circumstances and parties involved: 1. General Authorization: This is the most common type, granting broad permission for healthcare providers to disclose a patient's PHI for various purposes, as specified in the authorization form. It is often used for routine healthcare operations. 2. Specific Authorization: This type is more restricted and authorizes the use or disclosure of patient information for a specific purpose or to a specific recipient. For instance, a patient may grant authorization to share their PHI with a particular specialist for consultation purposes. 3. Authorization for Sensitive Information: In certain cases, highly sensitive information such as mental health records, HIV/AIDS diagnosis, or substance abuse treatment may require a separate and more explicit authorization due to the sensitive nature of the information disclosed. 4. Advance Directive Authorization: This type of authorization is used when a patient has provided directions in an advance directive, such as a living will or a healthcare power of attorney, stating their preferences regarding the use or disclosure of their PHI in the event of incapacitation or end-of-life care. It's important to note that the Kentucky Authorization to Use or Disclose PHI should be carefully reviewed by the patient before signing, ensuring they understand the purpose, scope, and potential consequences of sharing their medical information. Additionally, healthcare providers must strictly adhere to HIPAA requirements and maintain the confidentiality of patient information, ensuring it is only used and disclosed as authorized by the patient or as required by law.
Kentucky Authorization to Use or Disclose Protected Health Information (PHI) is a legal document that grants healthcare professionals the authority to share an individual's confidential medical information with third parties. This authorization ensures compliance with the Health Insurance Portability and Accountability Act (HIPAA), which protects patients' privacy rights and regulates the use and disclosure of PHI. The Kentucky Authorization to Use or Disclose PHI includes specific details about the purpose of the disclosure, the healthcare entities involved, and the type of information being shared. It requires the patient's explicit consent, usually obtained through their signature on the authorization form. This process allows healthcare providers to share an individual's PHI in situations such as coordination of care, billing and insurance claims, research studies, or legal proceedings. There are different types of Kentucky Authorization to Use or Disclose PHI, depending on the specific circumstances and parties involved: 1. General Authorization: This is the most common type, granting broad permission for healthcare providers to disclose a patient's PHI for various purposes, as specified in the authorization form. It is often used for routine healthcare operations. 2. Specific Authorization: This type is more restricted and authorizes the use or disclosure of patient information for a specific purpose or to a specific recipient. For instance, a patient may grant authorization to share their PHI with a particular specialist for consultation purposes. 3. Authorization for Sensitive Information: In certain cases, highly sensitive information such as mental health records, HIV/AIDS diagnosis, or substance abuse treatment may require a separate and more explicit authorization due to the sensitive nature of the information disclosed. 4. Advance Directive Authorization: This type of authorization is used when a patient has provided directions in an advance directive, such as a living will or a healthcare power of attorney, stating their preferences regarding the use or disclosure of their PHI in the event of incapacitation or end-of-life care. It's important to note that the Kentucky Authorization to Use or Disclose PHI should be carefully reviewed by the patient before signing, ensuring they understand the purpose, scope, and potential consequences of sharing their medical information. Additionally, healthcare providers must strictly adhere to HIPAA requirements and maintain the confidentiality of patient information, ensuring it is only used and disclosed as authorized by the patient or as required by law.