Oregon Sample Letter for Medical Authorization for Client Medical History
Description





How to fill out Sample Letter For Medical Authorization For Client Medical History?
Are you in the place the place you will need documents for both enterprise or specific reasons virtually every time? There are plenty of lawful file web templates available on the Internet, but discovering kinds you can rely on isn`t effortless. US Legal Forms delivers a large number of type web templates, such as the Oregon Sample Letter for Medical Authorization for Client Medical History, that are composed to meet federal and state specifications.
In case you are currently knowledgeable about US Legal Forms web site and get a free account, basically log in. Afterward, it is possible to download the Oregon Sample Letter for Medical Authorization for Client Medical History design.
Should you not have an account and need to begin using US Legal Forms, abide by these steps:
- Find the type you will need and make sure it is to the correct town/area.
- Use the Preview key to analyze the form.
- Browse the outline to actually have selected the right type.
- If the type isn`t what you`re trying to find, utilize the Research field to obtain the type that fits your needs and specifications.
- Once you find the correct type, click on Buy now.
- Choose the pricing prepare you would like, fill out the required info to create your account, and pay for your order utilizing your PayPal or charge card.
- Select a hassle-free paper structure and download your version.
Discover all of the file web templates you possess bought in the My Forms food list. You can aquire a more version of Oregon Sample Letter for Medical Authorization for Client Medical History any time, if needed. Just go through the necessary type to download or print the file design.
Use US Legal Forms, by far the most extensive collection of lawful varieties, to save some time and stay away from blunders. The support delivers professionally produced lawful file web templates that you can use for a variety of reasons. Generate a free account on US Legal Forms and initiate producing your daily life easier.
Form popularity
FAQ
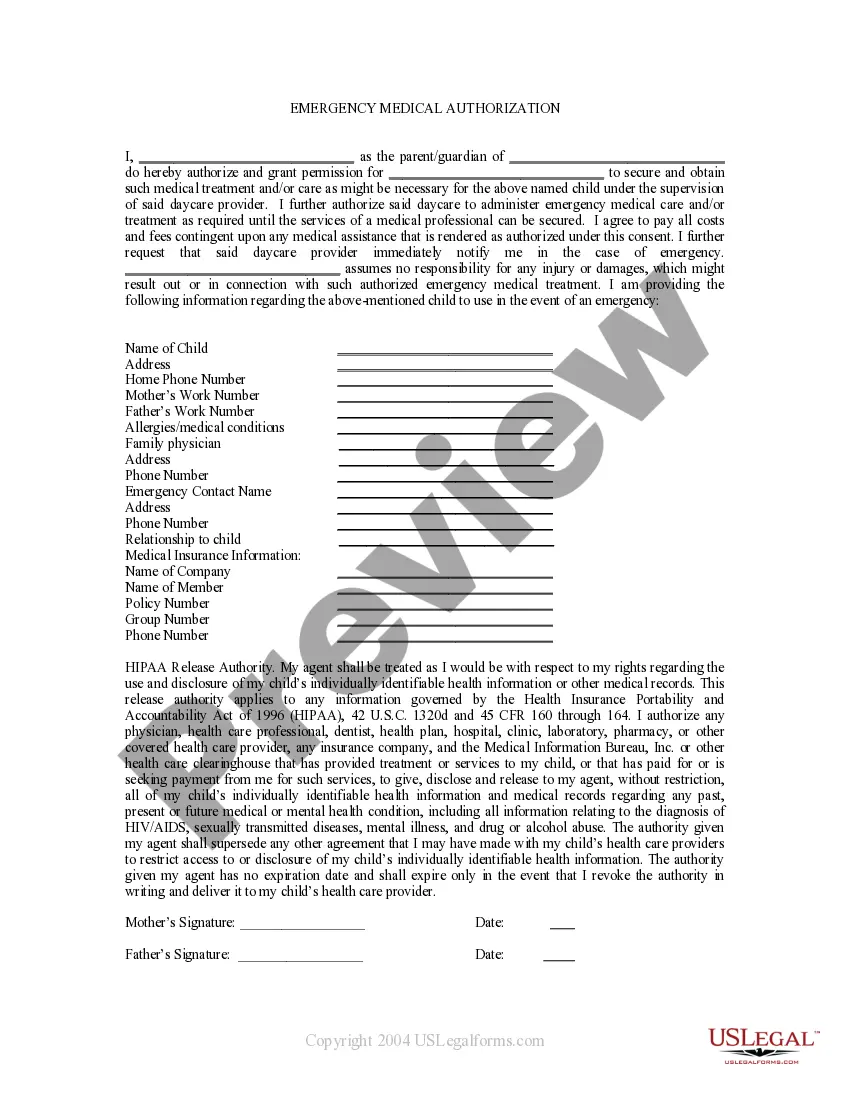
A HIPAA authorization form, also known as a HIPAA release form, is a document that individual signs for their health provider before the entity may use or disclose their protected health information (PHI). HIPAA authorizes the sharing of PHI for the following purposes: Treatment. Payment.
compliant HIPAA release form must, at the very least, contain the following information: A description of the information that will be used/disclosed. The purpose for which the information will be disclosed. The name of the person or entity to whom the information will be disclosed.
Patient Requests The patient's request must be in writing and must be signed and dated. ... The request must be directed to the provider who originated the portion of the record the patient wants to amend. The request must state which portion of the record the patient wants to amend and specify how it should be amended.
I was treated in your office [at your facility] between [fill in dates]. I request copies of the following [or all] health records related to my treatment. [Identify records requested (e.g., medical-history form you filled out; physician and nurses' notes; test results; consultations with specialists; referrals).]
Content for a valid authorization includes: The name of the person or entity authorized to make the request (usually the patient) The complete name of the person or entity to receive the protected health information (PHI) A specific description of the information to be used or disclosed, including the dates of service.
The key areas of focus are: Being clear on why you are writing the letter. Writing letters directly to the patient whenever possible. Using headings throughout the letter. Keeping the letter brief, clear, readable and relevant. Making sure that information is up to date, accurate and unambiguous.
A medical request form is a form used by healthcare professionals to request key information, treatment details, medication details, and more.
Here is how to write a request letter in 7 steps: Collect information relating to your request. ... Create an outline. ... Introduce yourself. 4. Make your request. ... Explain the reason for the request. ... Offer to provide additional information. ... Show your gratitude and conclude the letter. ... Use a professional format.