Oregon Authorization to Use or Disclose Protected Health Information
Description






How to fill out Authorization To Use Or Disclose Protected Health Information?
You can allocate time on the internet exploring for the legal document format that satisfies the national and state standards you desire.
US Legal Forms provides a vast array of legal forms that have been reviewed by experts.
You can easily download or print the Oregon Authorization to Use or Disclose Protected Health Information from my service.
In case you want to find another variation of the form, use the Search section to locate the template that meets your needs and requirements.
- If you already possess a US Legal Forms account, you can Log In and then click the Acquire button.
- Afterward, you can complete, modify, print, or sign the Oregon Authorization to Use or Disclose Protected Health Information.
- Each legal document template you obtain is yours indefinitely.
- To obtain another copy of any purchased form, go to the My documents tab and click the corresponding button.
- If you are visiting the US Legal Forms website for the first time, follow the simple instructions outlined below.
- First, ensure that you have selected the correct document template for the region/city of your preference.
- Review the form description to confirm you have chosen the correct type.
Form popularity
FAQ
You must get authorization from a person to disclose their protected health information when the disclosure is not permitted by law. This typically includes sharing information with third parties for purposes such as marketing or research. The Oregon Authorization to Use or Disclose Protected Health Information clarifies when consent is necessary, safeguarding the individual’s rights. Using services from providers like uslegalforms can streamline the authorization process, ensuring compliance with these essential regulations.
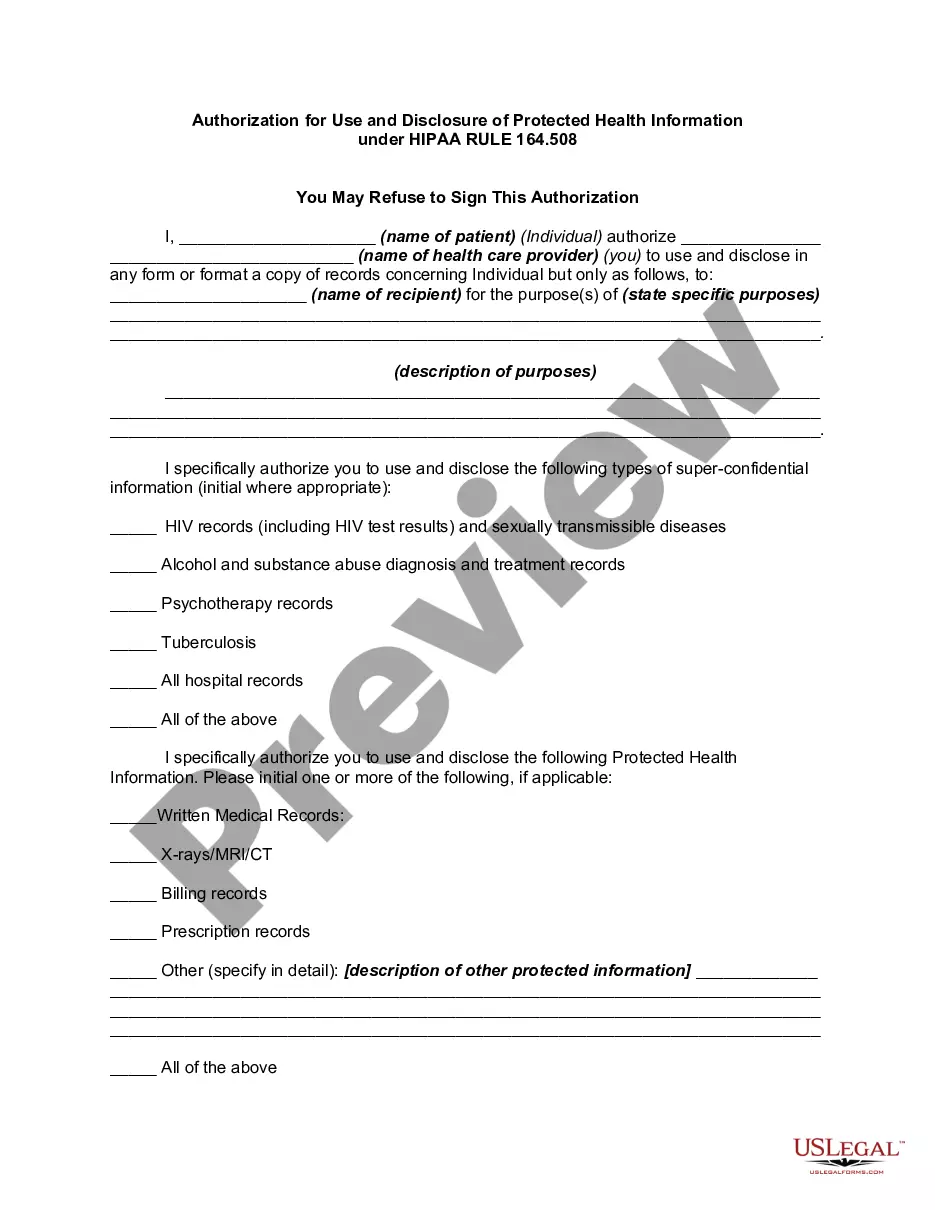
The authorization form for the release of protected health information is a document that allows individuals to give consent for their health data to be shared. This form outlines who can access the information and for what purpose, ensuring transparency in the process. The Oregon Authorization to Use or Disclose Protected Health Information is a crucial tool for managing your health records. Utilizing platforms like uslegalforms can help you easily obtain and fill out these authorization forms.
Unauthorized access, use, and disclosure of protected health information occurs when sensitive health data is accessed or shared without proper consent. This can lead to significant violations of privacy rights for individuals. The Oregon Authorization to Use or Disclose Protected Health Information is designed to prevent such occurrences by requiring explicit permission before sharing health information. By understanding these rules, you can better protect yourself and your health data.
U.S. Legal Forms offers user-friendly templates for obtaining the Oregon Authorization to Use or Disclose Protected Health Information. These templates simplify the process of creating legally compliant authorization forms. By using U.S. Legal Forms, you save time and reduce the risk of errors in your documentation. This ensures that you can focus on providing quality care while staying compliant with authorization requirements.
Under the HIPAA Privacy Rule, a covered entity must disclose protected health information in only two situations: (a) to individuals (or their personal representatives) specifically when they request access to, or an accounting of disclosures of, their protected health information; and (b) to the Department of Health
Generally speaking, covered entities may disclose PHI to anyone a patient wants. They may also use or disclose PHI to notify a family member, personal representative, or someone responsible for the patient's care of the patient's location, general condition, or death.
A HIPAA authorization is a detailed document in which specific uses and disclosures of protected health are explained in full. By signing the authorization, an individual is giving consent to have their health information used or disclosed for the reasons stated on the authorization.
Valid HIPAA Authorizations: A ChecklistNo Compound Authorizations. The authorization may not be combined with any other document such as a consent for treatment.Core Elements.Required Statements.Marketing or Sale of PHI.Completed in Full.Written in Plain Language.Give the Patient a Copy.Retain the Authorization.
What are two required elements of an authorization needed to disclose PHI? Response Feedback: All authorizations to disclose PHI must have an expiration date and provide an avenue for the patient to revoke his or her authorization. What does the term "Disclosure" mean?
Covered entities may disclose protected health information that they believe is necessary to prevent or lessen a serious and imminent threat to a person or the public, when such disclosure is made to someone they believe can prevent or lessen the threat (including the target of the threat).